Résumé
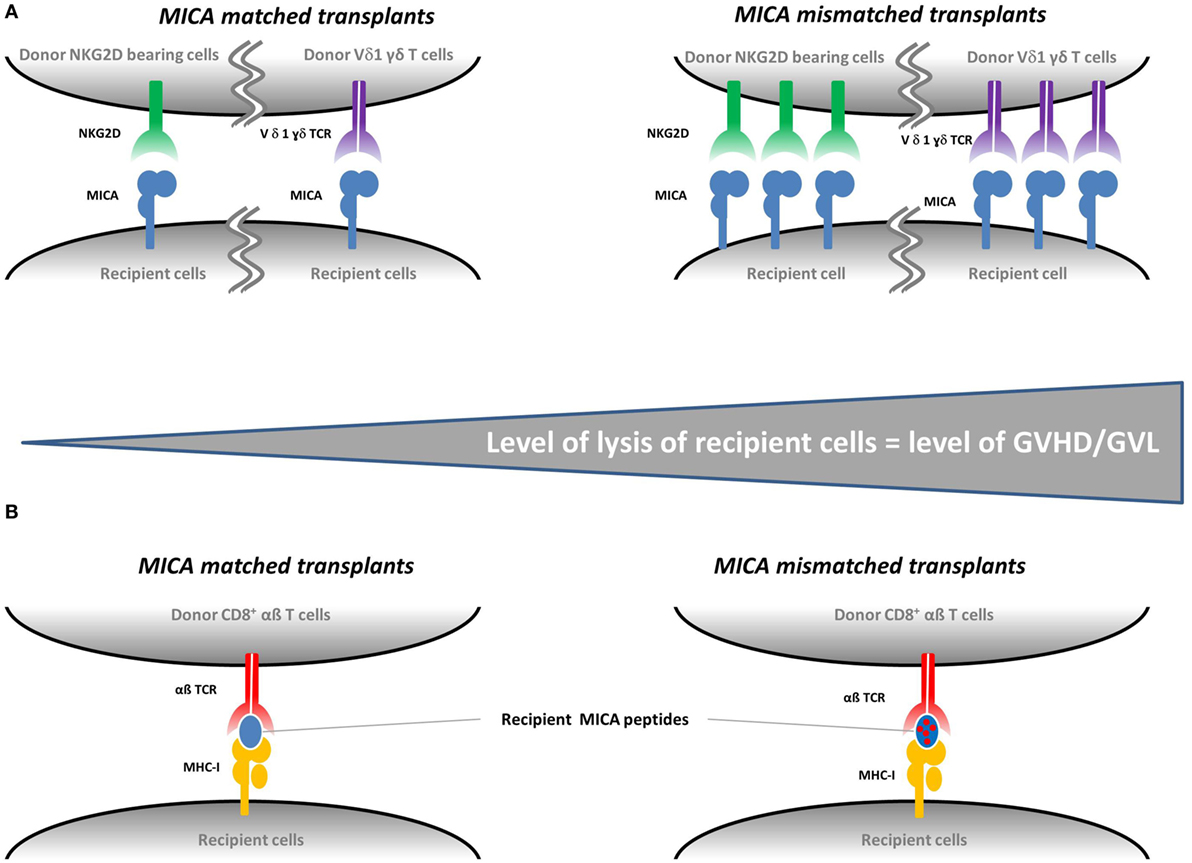
Natural killer group 2, member D (NKG2D) is an invariant activatory receptor present on subsets of natural killer and T lymphocytes. It stimulates the cytolytic effector response upon engagement of its various stress-induced ligands NKG2D ligands (NKG2DL). Malignant transformation and conditioning treatment prior to hematopoietic cell transplantation (HCT) are stress factors leading to the activation of the NKG2D/NKG2DL signaling in clinical settings. In the context of HCT, NKG2D-bearing cells can kill both tumor and healthy cells expressing NKG2DL. The NKG2D/NKG2DL engagement has therefore a key role in the regulation of one of the most salient issues in allogeneic HCT, i.e., maintaining a balance between graft-vs.-leukemia effect and graft-vs.-host disease. The present review summarizes the current state of our knowledge pertaining to the role of the NKG2D and NKG2DL in HCT.
Mars 2017 / Frontiers in Immunology – écrit par Carapito R, Aouadi I, Ilias W and Bahram S
Pour plus d’informations : http://journal.frontiersin.org/article/10.3389/fimmu.2017.00368/full